Research Titles
The GCSS Research Titles include abstracts. Full articles are not posted. Use MEDLINE (PUBWEB) the National Institute of Health’s database. Many chiropractic articles are not included in MEDLINE.
Full articles of titles that are found on MEDLINE can be ordered through LONESOME DOC. Useful search keywords: GONSTEAD, PLAUGHER G, ALCANTARA J, BACKACHE, CHIROPRACTIC.
Read a short Curriculum Vitae for GCSS Research Director, Roger R. Coleman, DC and GCSS Research Committee Chair, Mark A. Lopes, DC
The GCSS research articles have been broken down into seven categories.
GCSS RESEARCH LIST
Case Studies
Plaugher G, Bachman TR. Chiropractic management of a hypertensive patient. J Manipulative Physiol Ther 1993; 16:544-549.
Abstract:
Objective: Although many chiropractors may treat patients who have concomitant hypertensive disease, there is a paucity of literature on the nuances of case management for these patients. We report a patient who underwent a course of chiropractic care with a previous diagnosis of chronic essential hypertension.
Clinical Features: A 38 year old male presented for chiropractic care with complaints of hypertension, drug-related side effects and lower back pain. He was also receiving concurrent medical care for his hypertension.
Intervention and Outcome: The patient received specific contact, short lever arm spinal adjustments as the primary mode of chiropractic care. During the course of chiropractic treatment, the patient’s need for hypertensive medication was reduced. The patient’s medical physician gradually withdrew the medication over 2 months.
Conclusion: Specific contact short lever arm spinal adjustments may cause a hypotensive effect in a medicated hypertensive patient that may lead to complications (e.g. hypotension). Since a medicated hypertensive patient’s blood pressure may fall below normal while he or she is undergoing chiropractic care, it is advised that the blood pressure be closely monitored and medications adjusted, if necessary, by the patient’s medical physician.
Alcantara J, Plaugher G, Elbert R, Gatterman B. Chiropractic care of a patient with low back pain associated with subluxations and a Malgaigne-type pelvic fracture. J Manipulative Physiol Ther 2004;27(5):358-65.
Abstract
OBJECTIVE: To describe the chiropractic care of a patient with a pelvic ring fracture and concomitant subluxations of multiple segments of the spinal column.
CLINICAL FEATURES: A 23-year-old male, after falling down a flight of stairs, was initially hospitalized for fractures of the pelvis. Five weeks posthospitalization, the patient initiated chiropractic care with complaints of severe low back pain with lower extremity involvement. He also complained of neck pain and occipital headache. The patient had several positive low back orthopedic tests with bilaterally absent Achilles deep tendon reflexes. The anteroposterior radiographic view revealed ununited fractures at the left superior and inferior pubic ramus, noted as a type I Malgaigne fracture. Subluxations were detected at the left innominate (ie, fracture-subluxation) and at the patient’s lumbar, thoracic, and cervical spine.
INTERVENTION AND OUTCOME: The patient was cared for with contact-specific, high-velocity, low-amplitude adjustments to sites of vertebral and sacroiliac subluxations. The patient’s response to care was positive, receiving great pain relief. Less than 3 months after initiating care, the patient returned to work on regular duty.
CONCLUSION: There are indications that patients suffering from the injuries described above may derive benefits from chiropractic care. The practitioner must pay careful attention to issues of biomechanical and vascular stability and adjustment modifications in these types of patients.
Alcantara J, Plaugher G, Elbert R, Cherachanko D, Konlande J, Casselman A. Chiropractic care of a geriatric patient with an acute fracture-subluxation of the eighth thoracic vertebra. J Manipulative Physiol Ther 2004;27(3):E4.
Abstract
OBJECTIVE: To describe the chiropractic care of a geriatric patient with complaints of midthoracic and low back pain.
CLINICAL FEATURES: A 74-year-old woman sought chiropractic care with complaints of thoracic spinal pain following a fall. Palpation findings included hypertonicity and tenderness along with painful muscle spasms in the paraspinal musculature of the thoracolumbar spine. Limited range of thoracolumbar motion was found on extension and lateral flexion, most notably on right lateral flexion, with pain. Radiographic examination revealed a compression fracture at T8, in addition to spinographic listings. Signs of sprain injury were also detected at T8.
INTERVENTION AND OUTCOME: The patient was cared for with contact-specific, high-velocity, low-amplitude adjustments to sites of vertebral subluxations and at the T8 fracture-subluxation. The patient’s response to care was positive.
CONCLUSION: This case report describes the clinical features, care, and results of 1 geriatric patient with a thoracic compression fracture-subluxation treated with specific chiropractic procedures. The patient had an apparent decrease in pain as a result of the treatment. Due to the inherent limitations of a case report, it is inappropriate to generalize this outcome.
Alcantara J, Plaugher G, Araghi J. Chiropractic care of a pediatric patient with myasthenia gravis. J Manipulative Physiol Ther 2003;26(6):390-4.
Abstract
OBJECTIVE: To describe the chiropractic care of a pediatric patient with complaints associated with myasthenia gravis.
CLINCIAL FEATURES: A 2-year-old girl was provided chiropractic care at the request and consent of her parents for complaints of ptosis and generalized muscle weakness (ie, lethargy), particularly in the lower extremities. Prior to entry into chiropractic management, magnetic resonance imaging of the brain and acetylcholine receptor antibody tests were performed with negative results. However, the Tensilon test was positive and the diagnosis of myasthenia gravis was made by a pediatrician and seconded by a medical neurologist. Intervention and outcome. The patient was cared for with contact-specific, high-velocity, low-amplitude adjustments to sites of vertebral subluxation complexes in the upper cervical and sacral spine. The patient’s response to care was positive and after 5 months of regular chiropractic treatment her symptoms abated completely.
CONCLUSION: There are indications that patients suffering from disorders “beyond low back pain” as presented in this case report may derive benefits from chiropractic intervention/management.
Alcantara J, Plaugher G, Van Wyngarden DL. Chiropractic care of a patient with vertebral subluxation and Bell’s palsy. J Manipulative Physiol Ther 01/2004; 27(3).
ABSTRACT: To describe the chiropractic care of a patient medically diagnosed with Bell’s palsy and discuss issues clinically relevant to this disorder, such as its epidemiology, etiology, diagnosis, care, and prognosis. A 49-year-old woman with a medical diagnosis of Bell’s palsy sought chiropractic care. Her symptoms included right facial paralysis, extreme phonophobia, pain in the right temporomandibular joint (TMJ), and neck pain. Signs of cervical vertebral and TMJ subluxations included edema, tenderness, asymmetry of motion and posture, and malalignment detected from plain film radiographs. The patient was cared for with full spine contact-specific, high-velocity, low-amplitude adjustments (Gonstead Technique) to sites of vertebral and occipital subluxations. The patient’s left TMJ was also adjusted. The initial symptomatic response to care was positive, and the patient made continued improvements during the 6 months of care. There are indications that patients suffering from Bell’s palsy may benefit from a holistic chiropractic approach that not only includes a focus of examination and care of the primary regional areas of complaint (eg, face, TMJ) but also potentially from significant vertebral subluxation concomitants.
Alcantara J, Plaugher G, Klemp DD, Salem C. Chiropractic care of a patient with temporomandibular disorder and atlas subluxation. J Manipulative Physiol Ther 02/2002; 25(1):63-70.
ABSTRACT: To describe the chiropractic care of a patient with cervical subluxation and complaints associated with temporomandibular disorder. A 41-year-old woman had bilateral ear pain, tinnitus, vertigo, altered or decreased hearing acuity, and headaches. She had a history of ear infections, which had been treated with prescription antibiotics. Her complaints were attributed to a diagnosis of temporomandibular joint syndrome and had been treated unsuccessfully by a medical doctor and dentist. High-velocity, low-amplitude adjustments (ie, Gonstead technique) were applied to findings of atlas subluxation. The patient’s symptoms improved and eventually resolved after 9 visits. The chiropractic care of a patient with temporomandibular disorder, headaches, and subluxation is described. Clinical issues relevant to the care of patients with this disorder are also discussed.
Alcantara J, Plaugher G, Thornton RE, Salem C. Chiropractic care of a patient with vertebral subluxations and unsuccessful surgery of the cervical spine. J Manipulative Physiol Ther 10/2001; 24(7):477-82.
ABSTRACT: The chiropractic care of a patient with vertebral subluxations, neck pain, and cervical radiculopathy after a cervical diskectomy is described. A 55-year-old man had neck pain and left upper extremity radiculopathy after unsuccessful cervical spine surgery. Contact-specific, high-velocity, low-amplitude adjustments (i.e., Gonstead technique) were applied to sites of vertebral subluxations. Rehabilitation exercises were also used as adjunct to care. The patient reported a decrease in neck pain and left arm pain after chiropractic intervention. The patient also demonstrated a marked increase in range of motion (ROM) of the left glenohumeral articulation. The chiropractic care of a patient with neck pain and left upper extremity radiculopathy after cervical diskectomy is presented. Marked resolution of the patient’s symptoms was obtained concomitant with a reduction in subluxation findings at multiple levels despite the complicating history of an unsuccessful cervical spine surgery. This is the first report in the indexed literature of chiropractic care after an unsuccessful cervical spine surgery.
Alcantara J, Steiner DM, Plaugher G. Chiropractic management of a patient with myasthenia gravis and vertebral subluxations. J Manipulative Physiol Ther 07/1999; 22(5):333-40.
ABSTRACT: The chiropractic management of a patient with myasthenia gravis and vertebral subluxation is described. We discuss the pathophysiology, clinical features, and treatment of patients with these diseases. The 63-year-old male patient suffered from complaints associated with the disease myasthenia gravis along with signs of vertebral subluxation. The patient had an initial complaint of dysphagia. In addition, the patient experienced swelling of the tongue, nausea, digestive problems, weakness in the eye muscles, difficulty breathing, myopia, diplopia, and headaches. Balance and coordination problems resulted in walking difficulties. Contact specific, high-velocity, low-amplitude adjustments were applied to sites of patient subluxation. Myasthenia gravis is no longer debilitating to the patient; he is medication free and has resumed a “normal life.” The clinical aspects of the disease, including the possible role of chiropractic intervention in the treatment of patients suffering from myasthenia gravis, are also discussed. This case study encourages further investigation into the holistic approach to patient management by chiropractors vis-a-vis specific adjustments of vertebral subluxation.
Alcantara J, Plaugher G, Abblett DE. Management of a patient with a lamina fracture of the sixth cervical vertebra and concomitant subluxation. J Manipulative Physiol Ther 03/1997; 20(2):113-23.
ABSTRACT: To discuss the chiropractic management of a patient who sustained a unilateral lamina fracture of the sixth cervical vertebra. The patient had suffered cervical trauma from a motor vehicle accident. Clinical evaluation revealed acute global neck pain with associated left arm radiculitis and approximately 75% loss of useful left-arm motor function. The patient also complained of headache and low back pain. Computerized tomography and radiographic findings indicated a left lamina fracture of the sixth cervical vertebra. A rigid cervical collar was prescribed for the patient and specific-contact, short lever-arm, high-velocity, low-amplitude adjustments were applied at the levels of C2, C7 and L5, on different treatment visits, 11 days after trauma. The patient continued to wear the orthosis after each adjustment. The patient recovered from his injury and had no late biomechanical or neurological instability as a result of this management approach. The chiropractic management of a patient who sustained a unilateral lamina fracture of C6 with concomitant subluxations at C2 and C7 is discussed. This case study is the second reported in the scientific literature in which conservative chiropractic methods were applied to a patient with a lamina fracture.
Plaugher G, Alcantara J, Hart CR. Management of the patient with a Chance fracture of the lumbar spine and concomitant subluxation. J Manipulative Physiol Ther 11/1996; 19(8):539-51.
ABSTRACT: To document the chiropractic management of a patient who sustained a Chance fracture of the third lumbar vertebra. This case study represents the first report in the scientific literature of such an injury managed through chiropractic methods. An 18-yr-old man complained of low back pain and paresthesia in the lower extremities 10 days after suffering an automobile accident. Examination revealed a large circular edematous area from L1 to L4, tenderness to palpation at the L3 spinous process, reduction in global range of motion at the thoracolumbar region, and positive Lasègue and Kemp tests (bilaterally). Radiographic and computed tomographic scans revealed a Chance fracture of the L3 vertebra. The patient received specific-contact, short-lever arm spinal adjustments delivered primarily at L3 and L5, as well as bracing. Four months after initial treatment, the patient’s complaint of paresthesia had resolved and he suffered only occasional minor low back pain. The comparative radiographs demonstrate a reduction in the separation of the fracture fragments. A case report is presented of a patient who suffered a Chance fracture of L3. The patient was eventually managed by chiropractic methods including a specific contact high-velocity thrust procedure administered at the level of the fractured vertebra. The case represents the first known reporting of this type of chiropractic procedure applied to a patient with a Chance fracture.
Plaugher G, Alcantara J, Doble RW. Missed sacral fracture before chiropractic adjustment. J Manipulative Physiol Ther 10/1996; 19(7):480-3.
ABSTRACT: Reports of complications after chiropractic adjustments were administered to the lumbar spine and/or pelvis are rare. This case report provides the events associated with a sacral fracture that was not identified before a side-posture sacroiliac adjustment. The patient suffered from blunt, low back trauma as a result of a fall. Clinical evaluation indicated fixation dysfunction at the left sacroiliac articulation, with minimal edema/tenderness at the inferior portion of the left sacroiliac joint. Initial radiological evaluation failed to disclose the zone 2 sacral fracture because of an underexposed radiograph; thus, the patient was given a diagnosis of a sacroiliac sprain subluxation. A specific contact sacroiliac adjustment that uses the innominate as the short lever arm was administered to the patient in the side-posture position. Two adjustments were administered over 2 days. The patient developed sciatic pain after the second adjustment and subsequently referred herself to a medical orthopedist. Additional plain films were obtained, and a diagnosis of a zone 2 sacral fracture was made. The patient was prescribed bed rest; at 6 wk, her symptoms resolved and she returned to normal activity levels. Fractures of the spine and pelvis need to be considered in a patient who suffers blunt trauma. An adequate radiographic examination is necessary to make the appropriate diagnosis. Failure to diagnose the fracture may lead to complications, because the adjustment is not administered with regard to the biomechanics of the trauma or the actual clinical entity under scrutiny. This case study represents the first report of a complication after a sacroiliac adjustment in a patient who had a zone 2 sacral fracture that was missed in the diagnosis.
Clinical Trials
Plaugher G, Long CR, Alcantara J, Silveus AD, Wood H, Lotun K, Menke JM, Meeker WC, Rowe SH. Practice-based randomized controlled-comparison clinical trial of chiropractic adjustments and brief massage treatment at sites of subluxation in subjects with essential hypertension: pilot study. J Manipulative Physiol Ther 06/2002; 25(4):221-39.
ABSTRACT: To determine the feasibility of conducting a randomized clinical trial in the private practice setting examining short- and long-term effects of chiropractic adjustments for subjects with essential hypertension compared with a brief soft tissue massage, as well as a nontreatment control group. Randomized controlled-comparison trial with 3 parallel groups. Private practice outpatient chiropractic clinic. Twenty-three subjects, aged 24 to 50 years with systolic or diastolic essential hypertension. Two months of full-spine chiropractic care (ie, Gonstead) consisting primarily of specific-contact, short-lever-arm adjustments delivered at motion segments exhibiting signs of subluxation. The massage group had a brief effleurage procedure delivered at localized regions of the spine believed to be exhibiting signs of subluxation. The nontreatment control group rested alone for a period of approximately 5 minutes in an adjustment room. Cost per enrolled subject, as well as systolic and diastolic blood pressure (BP) measured with a random-0 sphygmomanometer and patient reported health status (SF-36). Pilot study outcome measures also included an assessment of cooperation of subjects to randomization procedures and drop-out rates, recruitment effectiveness, analysis of temporal stability of BPs at the beginning of care, and the effects of inclusion/exclusion criteria on the subject pool. Thirty subjects enrolled, yielding a cost of $161 per enrolled subject. One subject was later determined to be ineligible, and 6 others dropped out. In both the chiropractic and massage therapy groups, all subjects were classified as either overweight or obese; in the control group there were only 2 classified as such. SF-36 profiles for the groups were similar to that of a normal population. The mean change in diastolic BP was -4 (95% confidence interval [CI]: -8.6, 0.5) in the chiropractic care group, 0.5 (95% CI: -3.5, 4.5) in the brief massage treatment group, and -4.9 (95% CI: -9.7, -0.1) in the no treatment control group. At the end of the study period, this change was -6.3 (95% CI: 13.1, 0.4), -1.0 (95% CI: -7.5, 15.6), -7.2 (95% CI: -13.3, -1.1) in the 3 study groups. The mean improvements in the chiropractic care and no treatment control groups remained consistent over the follow-up period. This pilot study elucidated several procedural issues that should be addressed before undertaking a full-scale clinical trial on the effects of chiropractic adjustments in patients with essential hypertension. A multidisciplinary approach to recruitment may need to be used in any future efforts because of the limited subject pool of patients who have hypertensive disease but are not taking medications for its control. Measures need to be used to assure comparable groups regarding prognostic variables such as weight. Studies such as these demonstrate the feasibility of conducting a full-scale 3-group randomized clinical trial in the private practice setting.
Nansel D, Cremata E, Carlson J, Szlazak M. Effect of unilateral spinal adjustments on goniometrically-assessed cervical lateral-flexion end-range asymmetries in otherwise asymptomatic subjects. J Manipulative Physiol Ther 1989; 12:419-427.
Abstract:
A triple blinded, multiple-measure, experimental protocol was employed in order to investigate the effectiveness of unilateral cervical adjustments on goniometrically assessed cervical lateral-flexion asymmetries. On pretest, subjects selected for the experiments exhibited mean left-right lateral-flexion differences of approximately 14 degrees. In subjects which either received no intervention, or had been subjected only to preliminary palpatory and set-up procedures but no thrust, asymmetry magnitudes were found to be unchanged on goniometric post-testing done 30-45 minutes later. However, in subjects which received lower cervical adjustments performed on the side of most restricted end-range, there was a dramatic reduction in asymmetry magnitudes. Furthermore, the adjustment procedure used in this investigation appeared to be relatively side-specific, since adjustments, when delivered to the less restricted side, were only marginally effective in ameliorating the asymmetries. Potential clinical relevance as well as the possible structural or physiological mechanisms responsible for the results obtained in the study are discussed.
Nansel D, Peneff A, Cremata E, Carlson J. Time course considerations for the effects on unilateral lower cervical adjustments with respect to the amelioration of cervical lateral flexion passive end-range asymmetry. J Manipulative Physiol Ther 1990; 13:297-304.
Abstract:
The initial effectiveness as well as the temporal stability of the effect of cervical spinal manipulation with respect to the amelioration of goniometrically verified cervical lateral-flexion passive end-range asymmetry was examined. Responses of two groups of pain-free subjects were compared: a) those exhibiting end-range asymmetries of greater than 10 degrees who, in addition, had suffered previous neck trauma, and: b) those who happened to exhibit end-range asymmetries of greater than 10 degrees but who had no history of prior neck trauma. All subjects received a single lower cervical adjustment delivered to the side of most-restricted end-range, and goniometric reassessments were performed 30 minutes, 4 hours and 48 hours, following the adjustment. A dramatic amelioration of asymmetry was observed in both groups at 30 minutes and 4 hours post-manipulation. Furthermore, the magnitudes of these short-term effects were similar for the two groups. However, by 24 hours, a difference in the temporal responses of the groups had become readily apparent. By 48 hours, the difference was even more striking; whereas 14 of 16 of the subjects with no previous neck trauma continued to exhibit asymmetries of less than 10 degrees (mean +/- SEM = 3.8 +/- 1.0 degree), 12 of the 16 subjects with previous neck trauma had regained asymmetries of greater than 10 degrees (mean +/- SEM = 11.4 +/- 1.7 degrees). These results indicate that among asymptomatic (pain-free) individuals, the mere presence of passive end-range asymmetry as well as the magnitude of the short-term ameliorative effect of cervical manipulation do not distinguish these two categories of subjects. On the other hand, over long periods of time following manipulation, there appears to be a tendency of individuals who have suffered previous neck trauma to re-establish their aberrant cervical motion characteristics. The possible clinical relevance of these findings is discussed, and suggestions put forth regarding the definition of chronic cervical motion dysfunction. Possible mechanisms (e.g. spinal learning) which may be responsible for this condition are also addressed.
Nansel D, Jansen R, Cremata E, Dhami MSI, Holley D. Effects of cervical adjustments on lateral-flexion passive end-range asymmetry and on blood pressure, heart rate and plasma catecholamine levels. J Manipulative Physiol Ther 1991; 14:450-456.
Abstract:
The biomechanical and physiological effects of a single, unilateral lower cervical spinal adjustment delivered to the most restricted side of cervical lateral-flexion passive end-range were examined. Only healthy, asymptomatic male subjects who exhibited goniometrically verified lateral-flexion passive range of motion asymmetries of 10 degrees or greater on the morning of the experiment were chosen for the study. Post-treatment goniometric measurements revealed that in sham-adjusted controls, mean lateral-flexion asymmetries had not changed significantly during the 4 hour time period examined. However, in subjects who received lower cervical adjustments, dramatic ameliorations of asymmetry magnitude were observed which persisted throughout the entire 4 hour post-treatment time period. On the other hand, in the face of this rather robust biomechanical effect, heart rate and blood pressure measurements obtained at -60 and -15 minutes prior to treatments, and at 5, 30, 60, 120 and 240 minutes following treatments, revealed no significant differences between adjusted and sham-adjusted subjects at any of the time periods examined. Consistent with this, analysis of the plasma concentrations of norepinephrine, epinephrine and dopamine in serial blood samples collected at these times also failed to reveal significant differences between treatment groups at any of the time periods examined. The results of this investigation indicate that lower cervical adjustments are capable, at least in asymptomatic subjects, of inducing relatively robust biomechanical effects related to passive cervical end-range capability without simultaneously inducing significant alterations in the overall activity of the sympathetic nervous system.
Nansel D, Peneff A, Quitoriano J. Effectiveness of upper versus lower cervical adjustments with respect to the amelioration of passive rotational versus lateral-flexion end-range asymmetries in otherwise asymptomatic subjects. J Manipulative Physiol Ther 1992; 15:99-105.
Abstract:
The effects of cervical spinal adjustments delivered bilaterally either to the upper cervical region (C2-C3) or to the lower cervical region (C6-C7), were compared in groups of asymptomatic subjects exhibiting goniometrically verified left-right rotational or left-right lateral-flexion passive end-range asymmetries of greater than 10 degrees. Goniometric evaluation both prior to, and again within 30 minutes following treatments revealed that lower cervical adjustments were far more effective for the amelioration of lateral-flexion asymmetries than were upper cervical ones, whereas upper cervical adjustments were found to be more effective for the amelioration of rotational asymmetries than those delivered to the lower cervical region. These results are consistent with the view that passive movement restriction exhibited along the rotational axis is attributable to factors related primarily to the upper cervical region, whereas restrictions of passive movement along the lateral axis are more attributable to factors related to the lower cervical region. Further support for the regional independence of these axis-specific relationships is provided by similar results obtained in groups of subjects who happened to exhibit both rotational, as well as lateral-flexion, asymmetries of greater than 10 degrees on the day of the experiment.
Menke JM, Plaugher G, Carrari CA, Coleman RR, Vannetiello, L, Bachman TR. Likelihood-evidential support and Bayesian re-analysis on a prospective cohort of children and adolescents with mild scoliosis and chiropractic management. J Ariz Nev Acad Sci 2007; 39:99-111.
ABSTRACT
A previous study using frequentist analytic methods on a single cohort showed no difference in forty-one patients under chiropractic management for mild or early stage scoliosis. The grantor requested a re-analysis. Plain film radiographs of 41 children and adolescents were re-measured by Risser-Ferguson and Cobb methods. Three magnitudes and three types of change were constructed to cover various notions of scoliosis change: magnitudes of 1°, 3°, or 5°, and types that alternatively included or omitted no change as a possible successful outcome (arrested progression). Improvement was assessed from using three filters across three definitions of progression: 1) curve improved or stable, 2) improved only, and 3) those that either improved or progressed. Data were then analyzed by evidential support methods and Bayesian analyses at each filter and type of progression to establish whether improvement was likely attributable to treatment or spine characteristics. Intra-class correlation for intra-examiner stability was 0.73 by Cobb method. Reliability between the new and the previous examiner was 0.59 for pre- and 0.69 for post-treatment Cobb angles. Reliability increased dramatically when end vertebrae were specified. Ratio of number improved to those progressed to was at least 2:1 for all three levels of filter: 1˚, 3˚, and 5˚. Number of treatments or duration of care were not associated with improvement. However, the number of vertebral segments below the scoliosis curve apex – a measure of curve compression – and bone age accounted for 49% of adjusted R2 in Cobb angle changes. Initial Cobb angle as a clinical predictor was not supported. One treating chiropractor experienced a greater rate of improvement at the highest level of change (5°) in his patients. Results here could not be attributed to management, but could be from a type of scoliosis resolving spontaneously, or a subgroup of scoliosis cases that responded to chiropractic management or manipulation.
Overviews of Gonstead Technique
Cremata EE, Plaugher G, Cox WA. Technique system application: the Gonstead approach. Chiropractic Technique 1991; 3:19-25. (Authors’ abstract)
Plaugher G, Cremata EE, Cox WA. Letter to the editor; In reply. J Chiropractic Technique 1991; 3:134-135.
Plaugher G, Cremata EE, Cox WA. Letter to the editor, In reply. J Chiropractic Technique 1991; 3:135-136.
Plaugher G. Specific-contact, short-lever-arm articular procedures: advances in the Gonstead technique. In: Lawrence DJ, ed. Advances in chiropractic. Vol. 1, St. Louis: Mosby, 1994:341-372.
Lopes MA. Coleman, RR. Gonstead technique overview for Chiroaccess.com.
The Gonstead Technique was originated by Clarence Selmer Gonstead (1898-1978). Dr. Gonstead encountered chiropractic care when severe leg and foot pains, which were resistant to conventional medical care, responded to chiropractic adjustments. This event prompted Dr. Gonstead to seek a chiropractic education.
After graduating from the Palmer School of Chiropractic and Infirmary, Dr. Gonstead temporarily took over the practice of his chiropractic mentor before purchasing a practice in the now famous Mount Horeb, Wisconsin in 1923. Over the years, Dr. Gonstead developed the Gonstead technique which has been taught to thousands of students and doctors of chiropractic and also established the world famous Gonstead Clinic of Chiropractic in Mount Horeb. In 1974, after fifty-one years of active practice, Dr. Gonstead sold his clinic and passed away four years later in 1978. It has been said that Dr. Gonstead provided care to patients in over 1.2 million office visits in days that stretched up to twenty three hours of work.
The Gonstead concept of chiropractic begins with the body’s structural foundation and the intervertebral discs. Maximum balance and stability in the spinal column may be achieved when the pelvis, vertebrae, and legs are level. Foundational unleveling, intervertebral misalignments and motion disturbances, as well as nerve dysfunction, are primary considerations in Gonstead chiropractic health care and patient management. Injury to the intervertebral disc is of paramount importance in causing spinal subluxations, and therefore, Gonstead adjustments are designed for maximum affect to the discs, while also working to restore normal alignment and motion.
Gonstead chiropractic assessment utilizes several methods of examination to analyze multiple factors, which, as effectively as possible, uncovers the primary characteristics of intervertebral disc lesions, intervertebral and full spine and pelvis alignment, as well as neurological ramifications of vertebral subluxation and full body health.
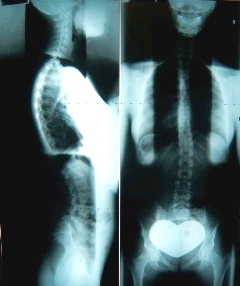
Full Spine Radiographs
The full spine radiograph is an integral assessment tool in the Gonstead system. Other important Gonstead examination procedures include static and dynamic palpation primarily of paraspinal bone structure and soft tissue, visualization of spinal motion, posture, gait and physical signs of inflammation near the joints, instrumentation such as para-spinal skin temperature assessment and other tools, which are used to examine all facets of the patient’s neuro-muscular-skeletal characteristics.

Differential Skin Temperature Meter
The full spine radiograph is analyzed with measurements drawn on the film to assess relative positions of the adjacent vertebrae and the pelvis region. These measurements translate into listings that the Gonstead chiropractor utilizes, along with other known variables about the characteristics of the subluxation, to direct the specific application of adjustment forces.
The Gonstead system uniquely emphasizes specificity, as it applies to which levels are being targeted for adjustments, both in the way the various aspects of alignment and motion disturbances are approached, and in the selection of which levels to adjust. Rather than a “shotgun” approach to care where any or all levels of involvement are adjusted on the same visit, Gonstead adjustments are directed at specifically selected levels of involvement for maximum restoration and balance of function. The notion of ‘primary’ versus ‘secondary’ subluxations, and subluxation versus compensation were largely developed by Dr. Gonstead. For every subluxation there is compensation. Further, certain subluxations will likely be exerting more influence on the overall bodily health status than others. Focusing spinal adjustments on primary subluxations is an important part of the Gonstead system of care.

Hydraulic Hi-Lo Table
Multiple types of tables are used for positioning the patient for Gonstead adjustments. The Hi-Lo table, with special modifications made specifically for Dr. Gonstead many years ago, has long been an integral part of the technique equipment, and accommodates a wide variety of patients, including pregnant women. The knee-chest table was one of Gonstead’s uniquely emphasized tables, to facilitate the posterior to anterior corrections of subluxation and reposition the posterior displaced inter-vertebral disc and can be used for the entire spine.

Lumbar or Pelvic Table Adjustment

Knee-Chest Table
The knee-chest table is also an excellent table to use for pregnant women. The Cervical Chair is used for most cervical spine adjustments, although prone cervical adjustments on the Hi-Lo or Knee-Chest or other prone tables are also performed in the Gonstead system.

Cervical Chair Adjustment
The Cervical Chair technique is one of the most unique types of Gonstead adjustments. Dr. Gonstead developed this technique to emphasize ‘lifting’ the vertebra in the cervical spine, as hyper-extension misalignment is common in this region. He discovered this approach by watching himself adjust under fluoroscopic imaging in his own facility, and was of the opinion that this was the only way to adequately adjust for hyper-extension misalignment in the cervical spine.
Gonstead adjustments can best be described as short lever, high velocity and low amplitude, with long lever assist force application. The short lever is the specific contact on the vertebra near or on the vertebral midline. The high velocity is the quick application of force. The low amplitude is the force depth being controlled at a shallow level, just enough to effect the disc and joint sufficiently. The long lever assist applies to the stabilization of the region above and/or below the contact area being adjusted, usually employing the chiropractor’s hand or thigh, not thrusting, but holding.
Another unique aspect of the Gonstead adjustment is the specificity of the contact point on the chiropractor’s hand. For the cervical chair adjustment, the distal-lateral-anterior tip of the index finger is most often used for C2 down to the upper thoracic vertebrae, as well as the analogous portion of the thumb for cervical chair Atlas contacts. Most other manual techniques utilize the broader areas of the metacarpal-phalangeal or inter-phalangeal joints for similar hand to vertebral contact points. The specific emphasis on the contact point for the Gonstead cervical adjustment enhances the specificity of the thrust in the line of correction, consistent with the goal of specific force application.

One Cervical Adjustment contact point
Although this technique was originated and clinically applied during an unprecedented and not since comparably repeated professional life by Dr. Gonstead, the Gonstead Clinical Studies Society (GCSS) continues the work. The GCSS conducts examinations for Diplomate status for qualified Gonstead practitioners. Qualifications include attending a sufficient number of seminars or other training hours in the technique, as well as Gonstead chiropractors receiving credit for teaching, publishing and other works related to the Gonstead technique. The examination consists of demonstration of detailed knowledge of the technique in both written and practical form, under the supervision of multiple Gonstead Diplomates.
While Gonstead practitioners have a strong base in the established chiropractic principles of the past, they also have a great interest in improving the abilities of future doctors of chiropractic. To that end, they embrace and support research that furthers the improvement of chiropractic care. The GCSS is a truly non-profit organization, with mostly volunteer efforts and a few paid positions contributing to the efforts of the group. Research and education are primary concerns with GCSS and every dollar that goes to GCSS is used to facilitate and support research and education in chiropractic. Further information concerning the Gonstead Clinical Studies Society may be found on this web site: www.gonstead.com.
Reference Sources for the Gonstead Technique
The following is a reference text, which expands on the basic fundamentals of the original Gonstead technique chapters that describe the Gonstead technique approach:
Plaugher G, Lopes M (eds). Texbook of Clinical Chiropractic, A Specific Biomechanical Approach. Baltimore: Williams & Wilkins, 1993.
The Gonstead Technique Chapters were the original resource of written material describing the Gonstead technique and are still available through the Gonstead Foundation at gonstead@mhtc.net:
Herbst RW. The Art and Science of Chiropractic. Sci-Chi Publications
There is also a Pediatrics textbook that uses the Gonstead technique as it primary approach to chiropractic care for children:
Anrig C, Plaugher G (eds). Pediatric Chiropractic. Baltimore: Williams & Wilkins. 1997.
Instrumentation
Plaugher G, Lopes MA, Melch PE, Cremata EE. The inter- and intraexaminer reliability of a paraspinal skin temperature differential instrument. J Manipulative Physiol Ther. 1991 Jul-Aug;14(6):361-7.
Abstract:
An experiment was undertaken to determine the intra- and interexaminer reliability of a paraspinal skin temperature differential instrument. 19 pain-free female chiropractic college students participated as subjects for the investigation. Three separate areas of the spine (C4-T2) and substantial agreement in the region T4-T8. The lumbar region could not be evaluated with he Kappa statistic due to limited variation. Following agreement for a positive finding in a given area, the numerical ratings were evaluated for agreement with the intraclass correlation coefficient (ICC). The first observation between examiners indicated fair agreement (ICC=0.2756, p=0.0478). The second observation between examiners had substantial agreement (ICC=0.6402, p=0.042). Intraexaminer agreement was moderate for one examiner (ICC=0.5078, p=0.0016). The other examiner showed an excellent level of agreement (ICC=0.8588, p<0.001) between observations.
Plaugher G, Haas M, Doble RW Jr, Lopes MA, Cremata EE, Lantz C. The interexaminer reliability of a galvanic skin response instrument. J Manipulative Physiol Ther. 1993 Sep;16(7):453-9.
Abstract
OBJECTIVE: To determine the interexaminer reliability of a protocol of use of a galvanic skin resistance device for detection of low resistance areas along the spinal column, in relatively pain-free subjects.
DESIGN: A blinded investigation of concordance of skin resistance examination findings over the spinal column using two clinicians experienced in the use of the instrument.
SETTING: A private practice chiropractic outpatient clinic.
PATIENTS: Sixty-four male and female chiropractic college students (mean age: 35 yr). The Visual Analog Pain Scale indicated a mean response of 7.6 mm on a 100-mm range.
INTERVENTIONS: None.
MAIN OUTCOME MEASURES: Concordance of examiners evaluated with the kappa statistic.
RESULTS: The results indicated modest levels of concordance for the first study sample (n = 46). The average kappa was 0.37. The second group assessed (n = 18) also demonstrated only modest levels of interexaminer concordance. The average kappa value for this sample was 0.36.
CONCLUSION: The use of the Electrical Conductor Scanner instrument for evaluating putative spinal pathology through manifestations in skin resistance in relatively asymptomatic subjects is not supported by the results of this experiment. The unevenness of data generated from this experiment in certain spinal regions necessitates further investigation prior to making any strong conclusions regarding the usefulness of this instrument in the clinical setting.
Plaugher G. Skin temperature assessment for neuromusculoskeletal abnormalities of the spinal column. J Manipulative Physiol Ther. 1992 Jul-Aug;15(6):365-81.
Abstract
OBJECTIVE: A qualitative review of the scientific literature on thermographic instrumentation for detecting neuromusculoskeletal abnormalities of the spinal column was made. Electronic infrared instrumentation (telethermography), liquid crystal thermography and various hand-held devices were scrutinized in terms of reliability and comparison with other diagnostic tests (e.g., computed tomography, myelography, electromyography, magnetic resonance imaging).
DATA SOURCES: A Medline literature search was performed from 1966 through 1990. English language material was retrieved using the following key words: thermography and spine, spinal injuries, cervical vertebrae, thoracic vertebrae, lumbar vertebrae, sacroiliac joint, lumbosacral region, back or neck. The Index to Chiropractic Literature was also reviewed. The categories of skin temperature and thermography were scrutinized. Chapters of texts and nonpublished works were not incorporated.
STUDY SELECTION: Studies involving the comparison of thermographic findings with those of other tests were the primary focus of the review. Case reports, as well as the use of thermography as an outcome measure, were also studied. Interexaminer reliability studies are reported.
DATA EXTRACTION: The study populations are characterized as well as binding procedures, if any. The authors’ statistical work, if applicable, is presented and criticized.
DATA SYNTHESIS: Relatively few reliability studies exist for thermography. Emphasis has been on validity studies that compare the results of the thermogram with other reference tests. There has been a general lack of high-quality research design (e.g., blinding) throughout the thermographic literature base. The sensitivity of the various thermographic instrumentation has shown encouraging results, although this must be tempered with the generally poor design of many studies. Specificity, in contrast, has shown mixed results. The review indicated telethermography to be a sensitive diagnostic procedure for detecting abnormalities, such as disc protrusion, of the lumbar and cervical spine. Liquid crystal thermography effectiveness is difficult to determine due to the paucity of blinded investigations, although normative data for the cervical spine and upper extremities is present. Literature on the various hand-held instruments has revealed moderate levels of examiner reliability for infrared devices, with less information available for thermocouple instruments. Normative data for hand-held instruments is absent.
CONCLUSION: Continued investigation is needed in the area of thermographic research in light of the paucity of blinded and/or controlled investigations. More sensitive neurophysiological and anatomical measures must be used when comparing the results from thermography. The lack of an available gold standard for comparing thermographic findings has been problematic. Future research should focus on thermography as a noninvasive outcome measure and interpreter reliability.
Letter to the editor:
Lopes MA, Coleman RR. Paraspinal skin temperature assessment rating incongruent with the data from studies. Chiropractic and Manual Ther (2013-11-27 04:00).
We found the article, “Review of methods used by chiropractors to determine the site for applying manipulation” by Triano et. al. to be, in many ways, very applicable and clinically important and we commend the authors on this accomplishment. However, there is a subjective nature to parts of the process involved in this review, which has led in our opinion to at least one inaccurate determination. We found the rating of ‘unfavorable’ applied by the authors to skin temperature assessment to be inappropriate, primarily based on the studies accepted for review by the authors.
The P.A.R.T.S. concept, described as a widely utilized method to justify treatment, was used as an integral part of this review and was the format for the sections in the article. The ‘T’ in P.A.R.T.S. stands for tissue temperature, texture, and tone.
In regards to the tissue temperature portion of this ‘T’ section, the authors stated: “The evidence from high quality studies is unfavorable toward the use of paraspinal skin temperature measures to locate the site of care, due to limited reliability.” We found this statement particularly interesting given that our study (1) was the top rated study by the authors in this category. We note that the authors generally refer to a range of findings of Kappa statistical values from our study, but do not mention the ICC values or the regional concordance differences or the differences between the first and second set of scans.
Instrumentation for paraspinal thermography is also one of the oldest methods of chiropractic assessment. Such instrumentation, including relatively new technology as with some of the instruments used in studies accepted for this review, has in most cases showed acceptable to excellent reliability as noted in the following articles reviewed by the authors:
Owens: “Intraexaminer and interexaminer reliability of paraspinal thermal scans using the TyTron C-3000 were found to be very high, with ICC values between 0.91 and 0.98. Changes seen in thermal scans when properly done are most likely due to actual physiological changes rather than equipment error (2).”
Hart: Reliability testing with 10 minute intervals between samples showed good ICC values of > 0.75 (3).
Roy: “…the infrared cameras showed that they were valid tools in a controlled environment (4).”
Plaugher, Lopes, et. al.: Following agreement for a positive finding in a given area, the interexaminer reliability of the first set of observations showed fair agreement with ICC values of 0.28. Intraexaminer agreement was moderate (ICC: 0.51) for one examiner and excellent (ICC: 0.86) for the other examiner. For the second set of observations between examiners the ICC values showed substantial agreement (0.64) and intraexaminer agreement was moderate for one examiner (0.51) and excellent for the other (0.86). Concordance measured with Kappa statistics were slight to moderate in the C4-T2 region and substantial in the T4-8 region. There was excessive overlap of the observations in the lumbar region, which contraindicated the use of Kappa statistics for that region (given a pre-requisite of some variation needed for Kappa), but this overlap more likely indicated high levels of interexaminer agreement in skin temperature differential findings frequently occurring at the same spinal levels (1).
Noting the range of possible determinations that could be applied to each procedure being reviewed, it appears that ‘unfavorable’ was not consistent with the evidence the authors accepted for their review. Here is the range of choices given by the authors:
“Favorable: For general use by clinicians to determine site of care
Favorable with limitations: Favorable for determining site of care although limits exist such as number and quality of studies, limited generalizability, etc.
Unclear: Based on the evidence available, it is unclear whether or not this procedure should be recommended for use
Unfavorable with exceptions: Procedure is not recommended for general use but may be used in limited circumstances
(e.g. other techniques unavailable.)
Unfavorable: Procedure is not recommended for use (limited number of studies, significant flaws in methods, not generalizable, high quality evidence against validity and/or reliability”
Triano et. al. mention that the unfavorable paraspinal skin temperature rating was based on “high quality studies” and since our study (1) was rated the highest and other studies on this subject showed favorable findings for reliability, it appears that the authors may have utilized our study as their primary source to opine that skin temperature assessment is unfavorable. Considering the findings of our study mentioned above in totality, the results were more positive than negative for reliability in our study, which leaves us with some confusion as to what Triano et. al. based a completely “unfavorable” rating on in regards to their conclusion.
The authors also seem to overlook the fact that various methods of skin temperature assessment exist. Contact thermocouple instrumentation is not the same as infrared thermography, which has shown very favorable reliability. The contact thermocouple instrument from our study in 1991, commonly known as a Nervoscope, was the original, non amplified version. There are now electronically amplified versions of that unit that need testing and it should not be assumed that one instrument study, no matter the quality, answers all questions about paraspinal thermography. Given the favorable results of the other paraspinal skin temperature studies utilizing different instruments and technology than ours, it seems those studies met the inclusion criteria and then were completely ignored in determining this rating.
We understand that there are some questions about the use of paraspinal skin temperature assessment: environmental controls, skin contact possibly affecting a reading or pattern, validity inadequately tested, etc. But many or most of the other assessment procedures deemed favorable in this study have similar questions about them.
There is enough data from the studies accepted for this review that show moderate to excellent reliability, however, that at least a conditional designation such as ‘favorable with limitations’ or ‘unclear’ should have been given for the paraspinal skin temperature assessment, although a ‘favorable’ rating appears more appropriate. The noninvasive nature of the assessment, lack of an expense burden to a patient, and a reasonable number of studies showing decent reliability should be enough to suggest this as a favorable assessment or at least unclear or favorable with limitations. Instrumentation thermography is close to a gold standard for this aspect of the P.A.R.T.S. concept.
Further, when comparing the designation of unfavorable for skin temperature assessment to tissue texture assessment (another part of the ‘T’ section), which was given a ‘favorable’ designation, we felt that tissue texture assessment proved to be no more or possibly less supported by the evidence presented in this review article than that presented for paraspinal skin temperature assessment. Tissue texture was listed as favorable based on only five studies, with three showing reliability of slight, fair and moderate respectively. It appears, therefore, that a more rigorous standard was applied to the paraspinal thermography than to tissue texture assessment.
Sincerely,
Mark A. Lopes, D.C.
Roger R. Coleman, D.C.
1. Plaugher G, Lopes MA, Melch PE, Cremata, EE. The inter- and intraexaminer reliability of a paraspinal skin temperature differential instrument. J Manipulative Physiol Ther 1991,14:361-367.
2. Owens EF Jr, Hart JF, Donofrio JJ, Haralambous J, Mierzejewski E: Paraspinal skin temperature patterns: an interexaminer and intraexaminer reliability study. J
Manipulative Physiol Ther 2004, 27:155–159.
3. Hart JH, Omolo B, Boone WR, Brown C, Ashton A: Reliability of three methods of computer-aided thermal pattern analysis. J Can Chiropract Assoc 2007, 51:175–185.
4.. Roy R, Boucher JP, Comtois AS: Validity of infrared thermal measurements of
segmental paraspinal skin surface temperature. J Manipulative Physiol Ther 2006,
29:150–155.
Radiography
Plaugher G, Cremata EE, Phillips RB. A retrospective consecutive case analysis of pretreatment and comparative static radiological parameters following chiropractic adjustments. J Manipulative Physiol Ther. 1990 Nov-Dec;13(9):498-506.
Abstract:
An investigation was undertaken to determine the effect of chiropractic adjustments on static radiological parameters. Standard plain film radiography was used. A retrospective consecutive case analysis approach was used for obtaining the data from the pretreatment and comparative posttreatment radiographs. Measurements for cervical lordosis, sacral base angle, lumbar lordosis, scapular angle, Cobb’s angle and retrolisthesis of adjusted lumbar segments were determined by marking films in a blinded fashion. Intra- and interexaminer reliability for the measurement of cervical lordosis and retrolisthesis were determined to be excellent with a low standard error (Pearson’s r range 0.89-0.97, p < .001 for cervical lordosis and Pearson’s r 0.74-0.90, p < .001 for retrolisthesis). The data from pre- and comparative post-measurements of retrolisthesis showed a significant reduction of approximately 34%. No reduction was seen in a control group with retrolisthesis. No pre/post comparative changes were observed with cervical lordosis angle, sacral base angle, lumbar lordosis angle, scapular angle or Cobb’s angle.
A. Letter to the editor; In reply. J. Manipulative Physiol Ther 1991; 14:335-336.
B. Letter to the editor; In reply. J Manipulative Physiol Ther 1991; 14:539.
C. Letter to the editor; In reply. J Manipulative Physiol Ther 1992; 15:331-332.
Coleman RR1, Lopes MA, Suttles RA. Computer modeling of selected projectional factors of the 84-in focal film distance anteroposterior full spine radiograph compared with 40-in focal film distance sectional views. J Chiropr Med. 2011 Mar;10(1):18-24.
Abstract
OBJECTIVE: The purpose of this study was to compare the 84-in focal film distance anteroposterior (A-P) full spine view to selected sectional views taken at a 40-in focal film distance for angles of divergence and changes produced by lateral translation and variation in source object distance.
METHODS: Computer models were used to determine angles of divergence and study the effects of lateral translation and changes in source object distance.
RESULTS: Lateral translation produced less projected axial (y-axis) vertebral rotation on the 84-in A-P full spine view than the film at 40 in. Angles of divergence are equal on the 14 × 17-in film at 40 in compared with the 84-in A-P full spine, and 70% of the 84-in full spine view is within the angles of divergence of the 40-in 10 × 12. The 84-in A-P full spine produced lowering and lengthening of the projected ilium when source object distance was reduced.
CONCLUSION: In this study, the 84-in A-P full spine produced less projected vertebral rotation on lateral translation. Its angles of divergence were greater than the 40-in 10 × 12 and equal to the 40-in 14 × 17-in film. Except for a 5.4-in section at both the upper and lower margins, the 84-in full spine view was within the angles of divergence of a 40-in 10 × 12. The full spine film produced projected ilium lengthening and lowering.
Plaugher G, Hendricks AH. The inter- and intraexaminer reliability of the Gonstead pelvic marking system. J Manipulative Physiol Ther. 1991 Nov-Dec;14(9):503-8.
Abstract
An investigation was undertaken to determine the inter- and intraexaminer reliability of the Gonstead pelvic radiographic marking system. This methodology analyzes the relative dimensions and spatial positions of the two innominate bones and sacrum and measures leg length inequality through an evaluation of femur head height. Two examiners marked 71 full spine radiographs twice to provide data from 284 analyses. Reliability was ascertained with the Pearson r, Spearman, intraclass correlation coefficient (ANOVA) and Kappa statistics. All results were statistically significant (less than 0.001) and indicated high levels of concordance. In every case, intraexaminer agreement was superior to interexaminer concordance.
Plaugher G, Hendricks AH, Doble RW Jr, Bachman TR, Araghi HJ, Hoffart VM. The reliability of patient positioning for evaluating static radiologic parameters of the human pelvis. J Manipulative Physiol Ther. 1993 Oct;16(8):517-22.
Abstract
OBJECTIVE: To determine the reproducibility of patient positioning on radiographically evaluated static configurations of the human pelvis.
DESIGN: Repeat anteroposterior radiography of the human pelvis was performed in vivo. Comparative examinations were performed after 1 hr in one subject pool. A second sample underwent repeat examination after a mean of 18 days.
SETTING: Outpatient private practice chiropractic clinic.
SUBJECTS: Thirty-seven relatively asymptomatic subjects participated in the experiment.
MAIN OUTCOME MEASURES: Millimetric evaluations were made for leg length inequality, right/left sacral discrepancies and right/left innominate differences. The null hypothesis was that the difference of the measurements from the two radiographs would be equal to zero. A paired t-test was used to analyze if there were any significant differences. The mean measured difference in millimeters and correlation coefficients were also determined for each variable.
RESULTS: Individual variations for several roentgenometric parameters, including leg length inequality and pelvic torsion, did not reach statistical significance (p > .05) although minor millimetric discrepancies were recorded. Correlation coefficients, in most cases, were relatively high.
CONCLUSION: A subject can be reliably positioned for repeat anteroposterior pelvic radiography for both 1 hr and 18-day intervals. The methodology described has applicability to full spine radiography when roentgenometric parameters of the pelvis are scrutinized.
Plaugher G. Letter to the editor; re: Gonstead Technique. Chiropractic 1991; 7:62.
Plaugher G. The role of plain film radiography in chiropractic clinical practice. Chiropractic Journal of Australia 1992; 22(4):153-161.
History Articles
Coleman RR, Wolf KH, Taylor J. The Gonstead Clinical Studies Society. Chiropractic History 2012;32:9-19.
The Gonstead Clinical Studies Society ROGER R. COLEMAN, DC*, KENNETH H. WOLF, PhD#, JEAN A. TAYLOR, DC**
*Director of Research, Gonstead Clinical Studies Society, croger1049@qwest.net
#Emeritus Professor of History, Murray State University
**Executive Director, Gonstead Clinical Studies Society and private practice of chiropractic, Santa Cruz, California
With the passing of Clarence Gonstead, DC, the chiropractic world lost a towering figure; however the vision of chiropractic that had been espoused by the iconic founder of the Gonstead Technique would not die. In an effort to maintain, promote and with time perhaps improve the vision of chiropractic that had been promoted by Dr. Gonstead, nine individuals stepped forward. On a spring day in 1979 this group met in San Mateo, California to form the Gonstead Clinical Studies Society. Over the next thirty years the organization has been a force in the education of both chiropractic students and practicing doctors of chiropractic as well as an avid supporter of research. At times the road has not been without its difficulties, but in a world marked by associations which rise and fall, the Gonstead Clinical Studies Society still stands proudly. A bond of fellowship based on mutual respect and dedication has been woven into a lasting tapestry that has withstood the test of time.
Coleman RR, Wolf KH, Lopes MA, Coleman JM. History or Science: The Controversy over Chiropractic Spinography. Chiropractic History 2013;33:66-81.
The historic year 1895 marked the beginnings of both radiography and chiropractic, inventions that would alter the course of world health care. These impressive developments are related in far more than merely dates of origin. Their histories have been intricately interwoven in a tapestry spanning over a century of impressive accomplishment. But these accomplishments have been accompanied by numerous internal conflicts within the chiropractic world. Techniques and ideologies have vied for supremacy over the course of chiropractic history. One controversy which continues today involves what at first may seem a relatively simple question: when or if to use imaging in a patient’s case. This seemingly innocuous problem has generated great debate and strife within the chiropractic community. The biomechanical based radiographers have embraced the historical chiropractic concept that the primary reason for ordering x-rays is to evaluate spinal alignment. The pathology based radiographers have rejected the traditional chiropractic approach and feel radiography should be performed in accordance with the “red flag” philosophy. Each group seems guided by its acceptance or rejection of historical chiropractic’s view on x-ray usage and then proceeds to craft arguments in line with a preconceived belief. It would appear that some tolerance might be expressed by both sides to allow individuals to practice somewhat to his/her own understanding without suffering the interference of either faction.